
Chapter One: Back Pain In Context
You Are Not Alone
Excruciating back pain is so seemingly unique and awesome an experience that the suffering individual often assumes that they are the subject of a rare event or perhaps one of the few persons to ever sustain such a degree of agony. After all, if it were a common phenomenon, surely someone they know would have told them about it. The reality is that few people actually discuss it because, in so doing, it exposes a frailty or imperfection in themselves. The ego rarely allows this revealing a disclosure.
Surprisingly enough, recurrent back pain is the most common complaint among adults approaching their physicians. It is second only to the common cold as a reason for office visits to primary care physicians. Low back problems affect virtually everyone at some time during their life. Surveys indicate that in any given year, 50% of working-age adults have back pain symptoms, but only 15-20% seek medical care. In one recent study, 41% of enrollees in a group health plan reported having back pain within the last six months. By the age of 70, 85% of the population will have had an episode of back pain. At any given moment, 15% to 20% of the adult population have low back pain. Back pain is the leading cause of disability in persons younger than 45 years, and the third leading cause among those older than 45. A number of studies have indicated that 40% of all adults will experience sciatica (back pain with radiation down the leg) some time during their life. In the U.S., 13.7% of all persons have back pain lasting more than two weeks. Lastly, back problems are the second most common reason for non-surgical hospital admissions among adults under age 65.
If money spent on a problem gives some measure of its extent in our society, the staggering costs and lost productivity are sufficient to convince the back pain sufferer that they are, indeed, a part of something big. The annual costs of disability and treatment of back pain increased from $14 Billion in 1976 to $30 Billion in 1986. By 1989, just the medical costs of back pain alone generated $14 Billion per year in the United States. The latest and most recent quote for the yearly costs related to back pain comes from the authors of the Agency for Health Care Policy and Research’s publication. They estimate it costs the health system upwards of $20 BILLION PER YEAR. In the U.S., back pain is responsible for an average of 12% of all sick leave, rivaling the common cold as a leading cause of absenteeism from work.
Back pain results in the loss of more than 93 million work days each year. It has been estimated that the yearly medical costs for treatment of just Lumbar disc disease is nearly $5 Billion., In the automobile industry, as much as 5% of a car’s price pays for back injury claims, and among postal employees, 1 in every 25 cents of postage pays for back problems. Tragically, back pain disables as many as 4 million persons in the United States per year.
Misery may love company, but delineating the magnitude of the problem offers small consolation for the individual back pain sufferer in the throes of agony. However, as Karma would have it, if spinal pain were not such a ubiquitous, inadequately addressed, problem in our society, this book probably would never have reached your hands. You are holding this book precisely because The O’Connor Technique ™ and the principles elaborated herein promise to favorably and dramatically alter the above statistics.
There is every reason to believe that, if put into wide-spread practice, The O’Connor Technique ™ has the potential to revolutionize the manner in which back pain is treated. By arriving at both a novel understanding of spinal mechanics and the development of a mechanism to physically alter them, most back pain can be successfully managed earlier and better than ever before. Prior to the onset of irrevocable damage, the deleterious consequences of neglecting spinal mechanical principles can be prevented, human movements can be directed to rectify anatomical discrepancies, and the environment can be altered to accommodate spinal anatomy rather than the inverse. Even though the evidence is not available to fully support this claim, I personally believe that practicing The O’Connor Technique ™ regularly throughout the aging process can prevent the crippling effects of kyphosis (the bent-forward posture of old age). Finally, by applying the knowledge presented in this book, its readers can expect to extract themselves from otherwise contributing to the horrific aforementioned back suffering statistics.
The Pain
Few people who do not have “bad backs” can appreciate the excruciating torture that constitutes back pain, the inconvenient agony of lying on the floor in a fetal position knowing that any movement produces a sensation equivalent to a sharp wedge being driven into the spine, the exponential number of lifestyle restrictions it produces, and the depression accompanying the realization that your mind has youthful desires yet your body’s actions are confined by limitations ordinarily reserved for the elderly.
Many cannot sympathize or empathize with back pain sufferers because they have never experienced the awesome reality of a pain so intense that they cannot lift themselves off the ground, let alone walk. A pain so oppressive that the simple act of freely breathing is denied, forcing one to take shallow breaths to avoid any extraneous movements. They cannot conceive of what it feels like to constantly search for a comfortable position where seemingly none exists. People, especially health care providers, who have not experienced this pain have no conception of this “task-master’s” incredible might. Back pain is so brutal and unforgiving that it exists only in the abstract to the uninitiated. Attempts to describe its magnitude by patients, if accurately done, are easily interpreted by others (physicians included) as an exaggeration for sympathy or histrionics for secondary gain. After all, nothing could hurt that bad!
Guess again unbelievers! I routinely hear stories from patients in which they describe being absolutely unable to move and only weakly able to call for help. One patient known to me sustained a fall in which she suffered a disc protrusion with spinal nerve root damage but the disc material recoiled back within the confines of the ligamentous capsule. Recently, she stood at the sink for an half an hour unable to change her position without agonizing pangs that shot through her back down to her legs. She had to be physically assisted to her bed by her mother. Adding literal insult to injury, she was adjudicated by the medical and judicial system to have psychological overlay that negatively influenced her ability to be helped, minor arthritis with a few osteophytes, and otherwise no evidence of significant back injury. Her tragedy was magnified by the “specialist” who couldn’t admit in his written procedure note that he failed in his attempt to properly perform a discogram on her (he stuck her unsuccessfully with a needle at least half dozen times). He, then, cleverly worded his findings (something to the effect that “no disc pathology could be identified”) which made it appear that she had no genuine pathology for the record. Therefore, no real physically demonstratable injury could be documented when she tried to sue the parties whose negligence was responsible for her fall. Compounding the physical pain she suffers, she also bears the psychic pain of experiencing that “the system” is so rife with injustice that it is hard for her to discern which is worse, the divine injustice of back pain or the societal injustice of a medical and courts system supposedly designed to prevent injustice.
As a consequence, any surgical option has been denied her because one doctor determined that her pain was largely psychological; and, yet another failed to diagnose it properly. The weight of these two opinions makes any surgeon reluctant to proceed without fear of a law suit should the results not meet expectations. Through my “hands on” manipulative technique, I could put her back “in”, but she, as of my last contact with her was unable to keep it in for any length of time. It is obvious by the relief that she gets with maneuvers that she has a mobile piece of disc material that is difficult to stay centralized; however, she cannot get this removed surgically because she has been determined not to be a surgical candidate. She is caught in a painfully surreal Catch 22. The pain she has experienced exists on levels far exceeding the physical realm, and she is probably forever limited to that relief which she obtains through practicing The O’Connor Technique™.
Contemporary Perspective
At this juncture, I suspect I am “preaching to the choir” because if you have picked up this book, it is most likely due to a personal experience with back pain or knowing someone close to you who can’t be faking that much discomfort so convincingly and consistently. Therefore, you probably know enough to understand that very little help can be expected from the current medical practices widely available to the back pain sufferer. After all, if you were largely satisfied with how you were treated, you wouldn’t have felt the need to acquire this book in the first place.
Not only myself, but other physicians categorize the current state of affairs as nothing less than “monstrous ignorance.” Dr. Paul Altrocchi, a neurologist in private practice told the Washington Academy of Family Physicians in 1987:
“In any group of people, we may find that 80% have had back pain at one time or another…yet few fields in medicine abound with such a monstrous amount of ignorance and lack of understanding.” The belief that the condition is a surgical disease is at the core of the myths surrounding back pain. This idea has come about because primary care physicians have for years, abdicated responsibility for these patients to others, he charged. “Back pain does not titillate our diagnostic minds, and it gives us complaining patients whose exams don’t lead to a wonderful sense of exhilaration.”(12)
It’s odd how back pain has gotten the “short shrift” in terms of the devotion of effort on behalf of the medical profession to analyze it to the degree necessary to properly manage it. I am constantly frustrated by how much pseudo-science is applied to the making of inaccurate diagnoses and prescriptions for illogical therapy. This is not solely my criticism but emanates from numerous other sources capable of publishing their objectivity. For instance, the medical journal, Emergency Medicine, anonymously reveals an attempt to rationalize a decision to abandon the time-honored requirement demanding that the physician make an accurate diagnosis before initiating treatment.
Figure 1; Excerpted headline from the 1993 medical journal, Emergency Medicine.
The article, “BACK PAIN, Is a Definitive Diagnosis Necessary?” begins:
“Vague associations between symptoms, pathologic changes and the results of history-taking leave primary care physicians no choice but to send patients with lower back pain home with no specific diagnosis. Many attempt to plug the clinical gaps with a progression of imaging studies. That route, however, is costly and sometimes misleading. But is an exact diagnosis really necessary in all cases of lower back pain? A Seattle physician thinks not. He believes that the goals of the history and physical examination should be somewhat less ambitious, aimed more toward the identification of more serious problems and the practical disposition (emphasis mine) of the patient.”
“The essential issues can be approached with the history and physical examination alone,” says Dr. Richard A Deyo, professor in the departments of medicine and health services at the University of Washington School of Medicine. “Only a minority of patients require further diagnostic testing.”(18)
The article, “BACK PAIN, Is a Definitive Diagnosis Necessary?” begins:
Sounds more like pragmatic disposal of patients to me. My wager is that the author has never suffered from a bad back, or he would be less likely to advocate diagnostic ignorance in order to search for a potential means to “dispose” of those who do.
Antithetically, the sagacious William Osler, M.D., in 1902, presciently answered this attitude by stating:
“In the fight which we have to wage incessantly against ignorance and quackery among the masses and follies of all sorts among the classes, diagnosis, not drugging, is our chief weapon of offense. Lack of systematic personal training in the methods of recognition of disease leads to the misapplication of remedies, to long courses of treatment when treatment is useless, and so directly to that lack of confidence in our methods which is apt to place us in the eyes of the public on a level with empirics and quacks.”
Whether originating from frustration, incompetence, or a desire to reduce medical expenditures, a willingness to abandon the necessity for a diagnosis reveals better than any other the current decision by medical intelligentsia to deviate from previous, held to be inviolate, standards. By way of comparison, if a patient with swollen ankles and shortness of breath asked a doctor precisely what was happening on a pathophysiological level, the doctor would, most likely, insist upon a battery of tests to make the diagnosis and justify its necessity with elaborate explanations involving sodium retention, serum renin levels, pulmonary wedge pressures, etc.; but just ask the doctor why, when you simply wake up in the morning, with no apparent trauma you have immobilizing neck stiffness or stabbing back pain, he will more than likely not give you a direct, competent, or anatomically sensible answer because it is as much a mystery to him as it is to you. The reality is that medical science has not really directed the equivalent amount of scrutiny to the back pain problem as has been devoted to other human diseases. When physicians attempt to educate patients as to the nature and means to a resolution of back pain in the absence of a diagnosis, they seemingly must be indulging in self-serving obfuscation apparently more illusional than realistically helpful.
An interesting study was recently done in which researchers educated physicians as to the state-of-the-art of back pain management; then, by telephone interviews of the patients these physicians subsequently treated, the researchers attempted to determine the success these physicians had in satisfying their patients desire to have their back pain “fixed.” The results were devastatingly dismal. The education program did not measurably affect outcome among any of the patients, including that subset of patients whose physicians had perceived themselves to have had the greatest benefit from the educational intervention!(19),(20)
I think this 1991 study, more than any other, exposes the failure of current medical management for low back pain. It would be comical if it were not underwritten in so much agony. Here, we are relying upon the most up-to-date minds in back pain management, educating society’s supposedly best and brightest, only to learn that, despite 62% of the providers believing that they had “acquired increased confidence” that they could help patients and 50% believing that they had “learned more” about the scientific and psychosocial aspects of back pain management, as well as 50% “feeling more comfortable” treating patients with low back pain, none of the patients got any better than they would have otherwise. One has to just shake one’s head and ask: “What is wrong with this picture?” It’s almost reminiscent of the finest and best-educated doctors in the 18th Century priding themselves upon having attended educational seminars on purging and bleeding and believing themselves to have arrived at the definitive state-of-the-art.
To be fair, there are other factors contributing to this complicated equation. There is also a great deal of physician trepidation in tampering with the spinal column in these days of litigation. If a doctor were to stray too far from the standard therapies and a paralysis were to occur, the next person he might be talking to would be that patient’s lawyer. Leaving well-enough alone and adopting a policy of “Less is More” (which is how the back pain gurus have interpreted and applied the overall message of the government’s guidelines discussed below) doesn’t appear so likely to result in nerve damage or paralysis for which an intervening physician can theoretically or legally be found culpable. No intervention, in that regard, is superior to one that might end the doctor in court when the outcome appears to be the same regardless of what any physician chooses to do. This philosophy updates the age-old physician’s precept, “first do no harm,” to the more contemporary, “don’t do anything outside of the guidelines and you won’t get sued.” This attitude appears to be well-received by doctors and insurance companies; unfortunately, it leaves patients suffering–a condition which seems to result every time bureaucrats try to practice medicine.
I intentionally delayed putting the book together until the definitive “state-of-the-art” was formalized in writing by way of the government’s new encroachment into medical arts referred to as Clinical Practice Guidelines: Acute Low Back Problems in Adults: Assessment and Treatment. Every physician in the country, one way or another, was going to be influenced by this promise to codify and justify back pain management (or better, “mis-management”); and I wanted to be sure that the state-of-the-art had been ultimately defined before I presented my method. I was not surprised to learn that nothing new is being really offered to the back pain sufferer by the government’s incursion (or academia’s dangerous collusion with same) into the realm of disease treatment.
Certainly, there was some advantage gained by assembling the country’s leading experts in an attempt to define the way a patient should be routed through the medical system; and I would encourage the reader to obtain the Agency for Health Care Policy and Research’s free publications related to: Acute Low Back Problems in Adults: Assessment and Treatment, by calling the information clearing house at 1-800-358-9295.
There are physician versions and consumer versions. They do at least a good job at defining dangerous back symptoms and signs as “Red Flags” indicative of a potential need for surgical intervention and differentiating these conditions from those amenable to “conservative treatment” (which, in truth, amounts to something more akin to neglect if one follows their advice). Nevertheless, the guidelines do serve an excellent function for my purposes. Their availability makes it unnecessary for me to reproduce all the work necessary to compile the existing literature or describe in detail the state-of-the-art in back pain management so that the readers may assess for themselves the available alternative methodologies. The reader can easily turn to those guidelines to determine what constitutes a potentially serious spinal condition. Any person satisfying those “Red Flag” criteria should probably not rely too rapidly or readily upon this methodology for their salvation until they have been reassured that they do not have a serious surgical condition. If so, they should insure that they present themselves to the most appropriate physician for evaluation before proceeding with any therapy. After exhausting all of the remedies outlined in the government pamphlets and provided through the current medical system, then, the reader may feel free to return to this website for advice and relief.
In delineating the current thinking on back pain, the guidelines prove, if only to my satisfaction, that no current literature seems to have arrived at as well-founded an explanation for the origins and solutions of spinal pain than is engendered in The O’Connor Technique ™. The careful reader of the government guidelines will note that in all their recommendations in favor of or recommendations against specific alternative methodologies, not a single one follows from “strong research-based evidence.” Therefore, it would seem unlikely that anyone could criticize myself for advocating my method; since the justification inherent in the government’s currently recommended modalities has arguably equivalent research-based scientific support as my own.
Actually, I should be content with that state of affairs. If all the answers were already available, there would have been little need for my book/website. No new revelations would be possible if the mysteries had been previously elaborated and the puzzle solved by someone else. One nice outcome of the government’s compilation of information is that manipulation therapy during the first month of symptoms was given some semblance of credibility by categorizing it as being justified with support by “moderate research-based evidence.” Since no mention was made of self-manipulation (which, if one were to characterize The O’Connor Technique ™ in its application by lay persons to their own back pain, it undoubtedly should be classified), it must, therefore, constitute a novel and unique classification.
Unfortunately, the manner in which these sort of governmentally-sanctioned pronouncements are received by the medical community tends to lend them an aura of “the final word” or becoming “written in stone,” leaving little or no room for innovation and an excellent means for a third party payor to refuse to pay for alternative medical strategies. One must understand that when the government decides to accomplish something, the impetus is politically motivated and controlled. With back pain, it appears to have gone something like this: The politically powerful and influential insurance companies would like to see less money spent on back pain. They monetarily support and acquire politicians who can control bureaucrats who then selectively employ and seat on committees only those professionals who espouse the desired medical philosophy that coincides with their monetary strategy. That way, the resultant conclusion appears to have been arrived at in an unbiased manner by objective experts. It’s an excellent societal management technique used by the ruling class for centuries to give the illusion that the very best is being done for the masses.
I fear that this current, government-sanctioned, justification for doing little or nothing for the majority of back pain sufferers a majority of the time will prevail; since, already, “The new thinking” on low-back pain concluding that “less is more” is severely limiting the use of needed imaging techniques by giving third party payers an elegantly documented means of denying approval for those modalities. I happen to especially advocate the use of imaging studies to document the reality of disc disease for diagnostic purposes, to ascertain the position of a displaced disc fragment, and to insure safety prior to ordering exercise-based physical therapy or active forceful manipulation. None of these governmental inquiries bothered to count all the people who got worse when they were sent out for manipulation or “work-hardening” exercise training in advance of a competent diagnosis.
Contrary to the prevailing recommendations, I have found imaging studies prove very self-helpful for insurance purposes. Immediately after an accident or other forcefully damaging event, I believe it behooves the sufferer to gain as accurate a piece of injury evidence as possible, since often, the only means of proof that can be obtained to justify a claim must be gathered while the damage is fresh before the disc migrates back into its central location either as a consequence of manipulation or random activity. On this issue, I heartily disagree with their findings and recommendations based upon the knowledge I have acquired through my own, albeit independent, experience.
The fact of the matter is, The O’Connor Technique ™ can be equally as effectively applied by an office-based physician to carefully but non-forcefully immediately alleviate acute as well as chronic back pain by a hands-on manipulative re-positioning of displaced, protruding or herniated disc material. Even after I teach them and they have shown successful ability, some patients nevertheless require intermittent assisted manipulation when they cannot get their own disc material back in place with The O’Connor Technique ™, requiring the repeated services of a trained practitioner. However, the government’s Clinical Practice Guidelines “recommend against” a “prolonged course of manipulation.” Does this give third party payers the justification they need to deny these services after an arbitrary period of time has elapsed? Does this imply that even prolonged courses of self-manipulation are not recommended? The originality of The O’Connor Technique ™ calls some of the most “modern” thinking into question. Principally, does what the government certifies as “ok” exclude all else and legitimize a denial of services or reimbursement?
I have been performing the type of manipulations arising from my unique understanding of back pain mechanics for several years now and have also arrived at a very simple assistant-mediated method which applies the principles of The O’Connor Technique ™ and may be practiced by any trained person to whom a back pain suffer turns for relief. This should probably be relegated to physicians or chiropractors so long as they are sufficiently educated to determine which patients are candidates for the technique and which ones should be referred to surgeons for last resort management.
Historical Perspective

Figure 2; Illustrations from the Canon of Medicine by Avicenna.
Using non-surgical, physically manipulative, means to mechanically alter the spine may be retrospectively looked upon, in part, as a long-lost art probably practiced by Medieval Arab physicians. The Canon of Medicine (Figure 2) by Abu Ali al Hussein ibn Abdallah ibn Sina (shortened to Avicenna, A.D. 960-1037), appears to have been instructing the 11th Century reader in a not unrelated method of back pain relief. It seems to me a method remotely related to The O’Connor Technique’s ™ application of traction accompanied by manipulation was most likely practiced a thousand years ago. In the absence of an anatomical foundation, these ancient practitioners may have been utilizing some of the basic components of what today I have independently developed as The O’Connor Technique ™. In the upper illustration of Figure 2, a board appears to be being used to forcefully hyper-extend the Thoracic spine. In the middle illustration, an extension technique is being combined with weighted pressure to forcefully hyper-extend the Lumbar spine. In the bottom illustration, the practitioner appears to be utilizing a mechanical traction device combined with an extension technique. It is not unreasonable to assume that the purpose was to mechanically remedy the same age-old problem that has plagued mankind since he began walking on two legs–the pain of a herniated disc.
In Indian Yoga, the practitioners appear to have realized centuries ago some benefit to be gained from adopting certain extension postures (Figure 3). Their efficacy was attributed to allowing energy to pour through opened nerve channels(21) and the effect, presciently claiming to exercise back muscles, “adjust any slight displacement of the spinal column, and relieve any backache caused by overwork,” constipation, flatulence, and utero-ovarial (sic) complaints.(22)

Figure 3; Swami Kriyananda adopting the Cobra (Bhujangasana) posture [with permission from Yoga Postures for Self-Awareness].

Figure 4; McKenzie extension exercise posture (Adapted from R. McKenzie).
Comparing Figure 3 with the McKenzie-type posture in Figure 4, seems to bear out this speculation; however, McKenzie (a New Zealand physiotherapist who devised a back pain program in wide-spread contemporary use) claims that he arrived at his method of centralizing disc material by accidentally leaving a patient in a similar posture for a prolonged period on his examination table only to discover that the patient’s back pain was resolved when he returned to the room. McKenzie further advanced this fortuitous finding into an exercise program with which many patients get relief from back pain.However, The O’Connor Technique ™ exponentially advances upon this age-old wisdom from the perspective of a medical doctor who has first-hand knowledge of the anatomical, physiological, practical, as well as theoretical aspects of back pain. This website seeks to impart this newly found wisdom to the back pain sufferer. The O’Connor Technique ™ rationally discards the harmful and logically incorporates the beneficial aspects of both the William’s and McKenzie techniques into a unified method that succeeds far beyond the limited benefits of either method taken individually.
I make reference to the McKenzie exercises because my initial reasoning that evolved into The O’Connor Technique ™ started with a different theoretical explanation of the origination of spinal pain than that proposed by McKenzie and because the manner in which McKenzie extension exercises claimed to centralize pain was inconsistent in alleviating my and others’ low back pain.
As an interesting and factual aside, before I came to the understanding engendered in The O’Connor Technique ™, I was helping some of my patients with a modified version of the McKenzie method (and meeting with limited success in stopping my own pain) and in my typical evangelical nature I presented it to my cousin who had all the symptoms of a chronically reducible disc herniation (that is, a piece of disc material that periodically went “in” and “out”.) When he attempted McKenzie extensions, he said they only hurt him more; and he related that the only way he could get relief was by lying on his side, assuming a fetal position, and forcefully pulling his head as close to his knees as possible. This was a technique similar to that described by William’s as effective; but I found that confusing because he was doing the exact opposite of the extension techniques and getting more relief. There had to be a rational explanation for why he got relief while accomplishing a bio-mechanically opposite activity. That caused me to return to the proverbial “drawing board” for the explanation of this conundrum.
When I independently looked, de novo, at the mechanical principles underlying the causes of back pain and examined them in terms of both the forces and actions resulting from those forces, I concluded that “over-stretching damage” to soft tissues of the spine (alleged to be the source of pain according to McKenzie(23)) were not the principle originating source for spinal pain. Rather, the pain comes from actual displaced disc material putting pressure on the ligaments surrounding the disc and disturbing the mechanical functioning of the disc unit. I assumed that this disc material had to have been displaced due to forces applied to the disc unit, and I reasoned that by reproducing the mechanical forces that caused pain in a reversed sequence, one could alleviate the pain using the individual’s anatomy as the tool to apply those forces. Lo and behold, it worked to alleviate my own back pain much more successfully and efficiently!
I ran into inconsistencies and more conundrums but held steadfastly to the belief that the mechanical processes of spinal pain were capable of being understood and reversed. When I found contradictions to my original hypotheses and events in the real world that didn’t fit my early beliefs, I reasoned out explanations. Where modification of my opinions were necessary by virtue of their being inconsistent with my observations or what patients told me of their experiences that weren’t consistent with the mechanics as I saw them, I was caused to revise my method to accommodate reality. I don’t feel this treatment of the subject perfectly answers the entire enigma of back pain, because I would be the first to admit that I do not have all the answers. However, I have solved enough of the mysteries to go public with what knowledge I have so as to be of enormous benefit to countless suffering people.
Science and Art
This medthodology is based upon the premise that there is nothing meta-physically mysterious about back pain. It is not only the result of fate but of function as well. By and large, once the mystery is revealed, the “secret” becomes common place and like all mysterious entities, it then becomes less frightening and manageable.
I have attempted to make this website readable for both the average person and referenced for the academic or professional. Despite my credentials as a physician and a University professor, I have elected an alternative method of presenting this to the academic world and documenting its success without controlled, peer-reviewed, “scientific” studies. Many academic professionals would prefer that new medical information originate from an orthopedist or neurosurgeon at the University level. In practice, educated as well as uneducated people fall into the intellectual trap of believing that the state of human knowledge has risen to such complexity that nothing can be of true value unless it originates from teaching institutions where knowledge is codified, structured, and monopolized. Such is not necessarily a fact.
Don’t misunderstand, I have deep respect and admiration for the theory and practice of science; however, there arise situations wherein the scientific process, as we have come to institutionalize it today, makes it sometimes inadequate for the study of human phenomena by its demand for absolute exactitude. If anything, the Heisenberg Uncertainty Principle (a theory holding that the more one attempts to study a phenomenon, the more one changes it simply by the observational act’s interfering with the true nature of the phenomenon) applies to some of the demands made upon the absolute adherence to scientific theory with respect to back pain because the process of observation is neither exact nor foolproof. I believe the manner in which back pain has been approached in this century fell victim to this reality.
The mechanically manipulative approaches taken by massage therapists, chiropractors, and ancient healers were often dispelled in their entirety by the medical establishment without looking to see if they had any basis in reality or attempting to discover the reason why they worked when successful.
In truth, I carefully observed a human phenomenon, acquired an in-depth understanding of the previously existent information base, found it inadequate, proposed countless hypotheses, tested those hypotheses, abandoned the non-reproducible components, formulated a theorem, then compared my observations and experiences against that theorem by testing, re-testing, and re-working the details. Admittedly, the knowledge came to me as much as by trial-and-error as what would be considered pure scientific inquiry. In spite of that, I am to the point where I feel I have arrived at a “truth” that constitutes a competent solution to an age-old-problem.
It also so happens that I have been in the unique position of having a population of back pain patients upon whom I was able to practice my technique and modify it accordingly without exposing patients to any mechanical forces or risks greater than that which would be expected from normal day-to-day activities. My own back also conveniently provided me with a willing and ever-present study group of one; but medical history is replete with major advances coming from competent observation of a single patient. Unfortunately, often, it seems, for anyone to be able to make even the simplest medical statement, it has to have been the product of a major, costly, project involving blinded study groups, control groups, and rigorous examination for statistical significance. I (as well as a large contingent of medical experts) have arrived at the conclusion that back pain has so many variables involved in its study that it is not always amenable to the usual methods of scientific inquiry.
For instance, if one were to attempt to compare so much as a single facet of The O’Connor Technique ™ with some other method in a controlled scientific fashion, it would be nearly impossible to eliminate what is called “bias.” One could never be certain that the person educating the patient populations did so properly and identically nor that the recipient of the information absorbed it uniformly or completely, was motivated to succeed, or remembered the details sufficiently to be successful. In advance, the researcher would have to have sufficient confidence in the method to be convincing to the patient (or else the advice might not be followed) and at the instant that was achieved, he would be guilty of injecting bias into the study. His inherent confidence in the method can be expected to alter his results by a projection of sincerity; otherwise, one would have to argue that patients could not be able to perceive nor would be affected by insincerity when the researcher had no idea whether his instructions would lead to benefit. Such constitutes the “art” of medicine as it applies to research.
I understand that, in medical science, sometimes as much as a third of the people get better as a result of the placebo effect. If another researcher were to be firmly convinced in the superior efficacy of an alternative method, a larger percentage of people might get better simply upon the strength of that researcher’s conviction that what he is doing will work. Also, in those people who were destined statistically to improve regardless of the treatment, they would be more likely to attribute the improvement to the alternative method regardless of its merit; otherwise the researcher would have had to have pretended to be neutral.
Also understand that many patients throughout medical history have gotten “better” despite therapies that ultimately were shown to have done more harm than good. Medical historians have ample examples of therapies that were so “effective” that they lasted for centuries only to be later shown to be worthless or actually more damaging. One would have to be biologically arrogant in the face of infinity to assume anything other than medical “science” still being in it’s infancy today. Future historians will probably have a comedic field day with what is currently acceptable medical practice.
Regardless, I can assure the reader of one fact, my life and the lives of countless numbers of my patients have been substantially bettered as a direct result of applying the principles of The O’Connor Technique ™. I have not failed to keep documentation on those patients that have walked into my clinic literally crippled with pain who achieved instantaneous relief when guided through the method and have been able to sustain that relief for prolonged periods. Certainly, not everyone achieves this dramatic level of relief; however, the overwhelming percentage of those people who I can define as having herniated disc material as the source of their pain do achieve remarkably favorable and reproducible results.
So as to test whether or not some would have achieved that relief anyway with a more well-established therapy, I withheld my method from a number of people and sent them through the usual orthopedic and neurosurgical routes. When they returned without relief, I then used The O’Connor Technique ™, and they were able to become pain-free. Now, I can’t, in clear conscience, persist in this practice because I would be denying them a valuable treatment for no apparent gain. This situation is reminiscent of the experiments that had to be stopped because the placebo control group was suffering so much that it would have been unethical not to give them the real treatment.
I have no doubt that The O’Connor Technique ™ can be superlatively effective in getting injured workers back to work faster, alleviate pain and disability more efficiently, and keep physically active people away from surgery more often and for longer periods than any existing back pain management program.
I have been developing this method for at least eight years and have been enormously successful with the patient population at my clinic. I know that the pain relief is not coincidental because it is too often dramatically immediate and most often in such close proximity to the start of therapy that no other explanation is suitable. I have followed these patients long enough to know that the relief is sustainable and recognized by the patients as valuable because they are so firm in their conviction that the method worked.
If a demand arises for documentation of this method’s success, I can simply return to the medical records for the appropriate analysis to prove my assertion. My records would be open to any researcher who legitimately wishes to verify or refute my claims. I am so convinced that The O’Connor Technique ™ works that I am reluctant to engage in the standard, costly, and time-consuming effort it takes to formalize the proof that is often demanded of others similarly situated. In reality, however, the success of this method will be demonstrated or refuted when large numbers of people begin to be helped by the techniques and the demand for the book or access to the website makes it obvious that the principles are genuinely therapeutic.
It is understandable for the potential reader to question the veracity of claims made by myself in this website. I’ve met with this attitude from celebrities who have back problems that are easily attributable to discs. They understandably believe that there couldn’t possibly be a better method than that prescribed by their own highly paid, University-affiliated specialist. Who can blame them? Their condition has been described to them in articulately specious terms, and they are convincingly reassured that they will be better in a reasonable period of time because the doctor is privy to the statistic that the majority of back pain is resolved within two months regardless of the method used. This statistic holds for The O’Connor Technique ™ as well; however, anyone using my method will find that usually the relief is instantaneous. There is no reason to wait weeks, months, or forever for random activity to possibly accomplish what my method does immediately and intentionally. Unfortunately, unless they have had the misfortune of being previously treated with some other method; they have nothing with which to compare my method.
For the individual or the study group, the obvious criticism of my intellectual process here would be: “How do you know that they wouldn’t have gotten better anyway just as rapidly with another method?” The answer I must resort to is my personal and professional experience both prior to my understanding the principles and after. Before I could genuinely help them, I was occasioned (like the over-whelming majority of doctors today) to watch them heal at their own pace, go from neurologist, to neurosurgeon, to physical therapist without definitive relief and continually get the same non-answers, veiled but never spoken assumptions of malingering, and with a frustrating inability to enjoy life as they knew it.
I distinctly recall one of the first patients upon whom I tried my method. He was a young man in his twenties unable to stand without a cane who bitterly complained about how his life was ruined and how he wanted to work but was sentenced to poverty because he couldn’t function with his back pain. He had been denied surgical relief because of no documentable nerve damage and his young age, but that didn’t change the fact that he was, for all intents and purposes, crippled. We both figured that he had nothing to lose. So, I gave my MANEUVERS a try on someone other than myself for the first time, and he actually walked out of the office without need of his cane. Within a month of following my instructions, he was able to seek work again. A few days later, I asked him if he thought my technique was responsible for his recovery or if he thought he would have recovered without it. He didn’t attribute his relief to chance nor consider his relief anecdotal (as I am certain my skeptical colleagues might readily point out). He was as convinced as I was that my method had achieved success where all else failed him.
Since then, I have been utilizing The O’Connor Technique ™ on everyone in whom I can define a discogenic (originating in the disc) source for back pain. I have made numerous modifications, toyed with some mechanically assisting devices, made certain that nothing posed a risk to the spinal cord or nerves with numerous imaging techniques, and followed numbers of people over long periods. The results have been so favorable that I had to publish the method.
I predict that in a short time, the method will become established therapeutic practice and evolve as things like that do. A therapist-assisted modification of this technique (like I do in my clinic) can be taught to the orthopedist, the primary care physician, or, yes, even the chiropractor so that within the space of an average office visit, the MANEUVERS can be administered to patients and immediate pain relief achieved where applicable.
I have evolved The O’Connor Technique ™ in the clinical/therapeutic environment to a point wherein mostly what I do with patients is verbally give them directions on the exam table and assist them in making their own movements in a controlled and protective setting. Their retention of the sequence allows them to practice the same techniques in the privacy of their own home, on household surfaces, at no cost, and whenever immediately necessary. I know this can be accomplished and taught to patients rapidly and effectively because I have repeatedly succeeded in this goal in my practice too often to attribute their immediate or rapid recoveries to happenstance.
I solidly understand that incorporating the principles and practicing the techniques described herein offers no guarantee that either I or the reader will not eventually have to resort to surgery. I accept the potential for my back to possibly get progressively worse as age-related changes occur, and the reader should consider likewise. Notwithstanding that concern, since I began using The O’Connor Technique ™, I have most certainly not gotten worse and have decidedly improved at a number of spinal levels that have to be considered “diseased.” Even though I have definitely improved, I accept that I have a good chance of re-injuring my back. With the prospect of relentless aging viewed as inevitable, I have every expectation for the on-going process to worsen, but I can say that I am certain that without understanding this method, my condition would have already progressively worsened to the point of surgery or incapacity. For nearly a decade, I have been able to avoid surgery and significant disability. Even if that were all this website could offer most back pain sufferers, I would consider it a resounding success.
Needless to say, I believe this method can do more than simply help people with existing back pain. If this method is practiced early enough in the course of disc problems, the relentless degenerative process can be forestalled and suffering prevented to the point of elimination, provided that the readers take personal responsibility for their problem and make the necessary modifications in their activities of daily living to positively affect their destiny.
Alternative Therapeutic Modalities
There are certainly other back pain therapies available; and I would invite the reader to try them. They are usually divided into conservative and surgical modalities. For an overview of the available modalities, I again refer the reader to the above referenced AHCPR literature or any practitioner.
In short, the conservative model usually involves any number of physical therapies which can be summarized best in a single sentence:
“There’s no evidence that typical physical therapy in the form of ultrasound, hot packs or heat make any difference at all. Asking a patient to spend a lot of money on various approaches is unwarranted.”(24).
I couldn’t have said it better. In fact, if I’d have said it first, the reader might think I was self-servingly trying to coax people into believing that my method was the only path to relief.
The purpose of this website is not to evaluate the merits of all the available therapies; however, it would be incomplete unless I gave some direction to those who’s back pain is not alleviated by this method and are forced to seek other relief from pain. I do not believe that my method will solve everyone’s pain; so, for those instances, I have a duty to offer some of my perspectives so that at least some pitfalls can be avoided. After all, I have been forced by my own back pain to consider all the options. Who better can lend that personal touch to the experience?
Surgery
If the reader is considering the alternative surgical option and turns himself over to a surgeon for a solution, I must first reveal a sobering statistic. In a study by Weber(25), 280 patients were evaluated over a ten year period. At the end of one year, 90% of surgical patients reported a satisfactory outcome compared with only 60% of the conservatively treated group. However, 25% of the conservatively treated group over the ten year period resorted to surgery. At ten years, this difference disappeared, indicating that surgery is initially helpful but the outcome at the ten year point is largely the same with or without surgery. Revealing another interesting statistic, 40% of conservatively treated patients are not satisfied as much as ten years later. This would seem to indicate that, over the long term, state-of-the-art management (surgical or conservative) fails to satisfy at least 40% of back pain sufferers.
When comparing the efficacy of non-surgical versus surgical management of disc disease, no significant difference in recovery of function has been reported between patients whose herniated discs resolved spontaneously and those whose herniated discs were surgically removed.(26) However, when using my method, the relief achieved cannot be considered spontaneous. It will come, if it does, as a consequence of directed therapy, the proof being in the rapidity of relief, in most cases. The future will determine how successful The O’Connor Technique ™ is when it is compared against surgical intervention; my conviction is that it will be found superior in the long run.
It is with this thought that I temporarily abandon discussion on surgical remedies until the reader has had a chance to acquaint himself with the terminology of the disc, its anatomy, and pathology. At this point, my intention is to give an alternative to surgery and only after having exhausted the opportunities offered through The O’Connor Technique ™ should surgery be realistically considered.
Comparative Programs
Although there are several back pain books on the market and numerous physical therapy programs, The O’Connor Technique ™ is not just another back pain methodology filled with various exercises that no one can realistically be expected to do when in the throes of a back pain episode or for that matter maintained daily for the rest of one’s life. It differs substantially from any other previously described program in that it advances an entirely novel method of back pain management. The major difference between The O’Connor Technique ™ and conventional, traditional, exercise therapy is that this technique doesn’t simply hand out a number of instructions that are assumed to be helpful without giving a rational, specific, physiological and anatomical justification. In my opinion, the back and neck exercises advocated by pre-existing literature and prescribed by most physicians as “physical therapy” have no true direction or sense to them because among other failings, they are not diagnosis-specific nor do they consider the physical realities of the individual. Doctors prescribing them, today, attempt to “sell” the impossible “one remedy that cures all”. While ignoring the necessity for specificity, upon which they so often pride themselves when dismissing any therapy which originates outside of academia, they, in essence, commit the same fault for which they so often criticize alternative therapists. If you don’t believe this, ask the doctor who has prescribed physical therapy for your back pain exactly what mechanical principle he/she is relying upon and what specific instructions he/she is giving to the physical therapist relevant to your particular back pain. Then, compare that answer to the explanation you would get if you sought the same answers from this treatment of the subject. My bet is that you will find a much more cogent and sensible rationale in this material’s prescription.
That is not to say that some physical therapy programs don’t have successful outcomes. In fact, this method is a “physical therapy;” and it would be absurd to argue that physical therapy has no benefits. However, just as throwing virgins into volcanoes had been shown to effectively stop the Polynesian lava flows, so too, the exercise programs of the past tell you to do certain things that from time to time appear to be effective. If they are practicing the current state-of-the-art, their “effectiveness” is more likely the consequence of random chance and probability than directed, intelligent, common sense effort. After reading this website, I can pretty much guarantee that the reader will agree with me.
It makes very little sense when a disc is “out” to commit the same, identical, movement (under the auspices of an exercise) that put it “out” in the first place, even in small increments. Unless of course, they wish to verify the principles of homeopathy in which a small amount of poison that produces given symptoms is a means of curing a disease with the same symptoms. I don’t think so. I think that even a little damage repeated many times cannot be expected to lead to consistent improvement.
One patient, I recall, described a series of neck exercises that she ritualistically performed every morning which seemed to make her functional yet did not even approach what could be looked upon as relief. They consisted of sequential side-to-side and rotatory movements of the neck. She was suffering from an off-center disc to the left in the C2-C3 level. So, every time she tilted her head to the right, she actually aggravated the problem. The relief she did seem to get was only because her ritual ended with a twisting movement after a left-sided flexion. Had she not coincidentally or by unconscious trial and error finished with that physical set of forces she would have received only pain for her effort. In her case, it only gave a modicum of relief which was to say she was in pain most of the time. When she began applying The O’Connor Technique ™ she immediately, that is, the next day, began appreciating what it was like to live without pain again.
The O’Connor Technique ™ relies upon a few basic, easily understood, principles, within the parameters of which any spinal activity can be evaluated as favorable or unfavorable. For instance, this method does not allow intentional WEIGHT-BEARING flexion of the spine at the painful site. For the Lower Thoracic and Lumbar spine pain sufferer, that eliminates any type of sit-up type exercise often advocated in other back pain management programs and literature wherein a supposition is made that increasing abdominal tone is essential to the restoration of a normal spine.
Take, for instance, the Williams exercises designed by the same-named orthopedist, repeatedly recommended through the years by countless doctors, and still in wide-spread use since at least 1974 for low back pain.(27) They would have the back pain sufferer repeatedly engage in weight-bearing flexion of the spine which causes a disc condition to actually get worse. I’ve yet to figure out how they ever gained popularity in the medical profession. I suspect they were and are still offered as a “something” in place of the alternative “nothing.” They apparently are statistically tantamount to ignoring the problem because the patients tend to eventually get better whether they are practiced or not. Nevertheless, they were and seemingly are still one of the standards of practice, since they continually and repeatedly are recommended in the current literature as well as by many primary care physicians, orthopedists, back pain educators, and physical therapists. Chiropractors rarely offer them because if anything worked at home, it might serve to keep patients out of their offices–they are seldom given to cutting their own economic throats. Besides, Williams exercises have never been proven to be effective.(28),(29) In a limited regard, as it pertains to extension exercises, I would contend that The O’Connor Technique ™ can be seen to be consistent with some components of most other back pain exercise programs. Exercise, in and of itself, is not bad; but it becomes maladaptive when it is not rationally based.
If the exercise program doesn’t insure that no further damage is done by the process, then it is counter-productive. The absurdity of any exercise prescription given to an acutely injured back patient is made manifest any time that the doctor cannot accurately diagnose the lesion and insure that the exercises will not increase the damage. In the case of extension versus flexion exercises, a certain percentage of patients will get relief with either method owing to the varied disease states encountered by chance and probability; however, simply because a quantifiable number of people get relief doesn’t justify increasing the pain of a probably larger percentage of those in whom a given exercise is decidedly inappropriate.
The test of any medical therapy is that it proves to be safe and effective. The currently available exercise regimens prescribed in other programs for low back pain, in part, can be seen as effective if they contain extensor strengthening components, but cannot be considered safe if they include weight-bearing flexion.
The closest analogy I can draw to what is being given to back patients today with most physical therapy prescriptions is the same as if a patient were to walk into a doctor’s office stating that he had a “blood pressure problem” and having the doctor offer two different pills. One pill makes the blood pressure go up and the other brings it down. The doctor then plays an “eenie-meenie-miney-moe” game and randomly gives the patient one of the pills. A higher understanding and logic tells us that most people are going to need the pill that brings down the blood pressure, and about fifty percent of the time the doctor will be “right.” Unfortunately, an equal percentage of patients will not only be not helped but even harmed, by the wrong pill.
Certainly, after the pill takes effect, determining whether the patient’s blood pressure goes up or down will offer some measure of information as to whether the truly correct decision was made; but that policy necessitates that the answer comes only after the prescription is administered and its expense and consequence is felt. In the context of a back pain exercise prescription, the incorrect choice is felt in both the patient’s increase in pain and the nonproductive dent in his wallet. This method is predicated upon the assumption that these are two consequences that most people would rather do without if there is a better way of proceeding.
I would hope that most intelligent patients would argue the inadequacy of the analogy from the perspective that the doctor should have most certainly first measured the patient’s blood pressure to determine the true nature of the problem before initiating a prescription. In the context of back pain, the doctor would, similarly, have been expected to first determine the precise nature of the back pain’s origin before writing his prescription. However, one must understand that the principle means a doctor has of correctly diagnosing a disc problem (in the absence of applying The O’Connor Technique’s ™ methods to determine if the back pain’s origin is discogenic) is with an objective measurable imaging study. Those have been deemed too expensive by the current “back pain intelligentsia” in the absence of clinically obvious nerve damage; and, even when they show a disc bulge, the artificially erudite clinicians will most likely quote a study that claims such a finding is present in too many supposedly asymptomatic people to be the source of the pain. So, the “eenie-meenie” game is played with exercise prescriptions because there is usually a failure to diagnose the disc as the source. Then, currently acceptable exercise regimens are prescribed without the knowledge necessary to logically presume how, or if, they will be successful.
I refuse to play that game. This website gives the readers explicit means by which to determine for themselves what logic-motivated type of movements or exercise program should be employed and the physiological time an exercise program can begin based upon mechanical reality.
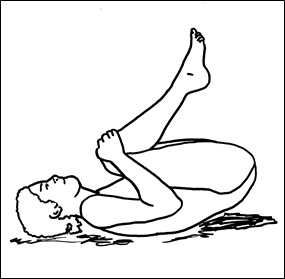
Figure 5; Exercise involving painful discs in flexion and bearing the weight of the legs while abdominal muscles are contracted.
I would argue that the currently advocated exercise regimens are one of the major reasons why our present back care management strategy is in such obvious disarray. Williams’ and McKenzie’s exercises have had years to competently address the problem and reduce back pain; yet they still leave the back pain sufferer today with the same statistically dismal chance for relief as they had for years in the past. One reason is simple: They often actually reproduce the forces that caused the injury and ask the sufferer to repeatedly perform them.
Too, they usually are prescribed in a progressively increasing and complex series so as to give the illusion of scientific accuracy; when in actual practice, if you are not the ideal candidate, the more you do, the worse you will get. Like so many of my patients, I tried them before I developed my alternative. I, too, abandoned them because they hurt too much and seemed to make me worse.
In the section discussing weight-bearing flexion, the demonstrations why these type of exercises can be harmful are discussed and the specific exercises that should be avoided are described. Here, it is sufficient to say that those components of the McKenzie or Williams exercises that involve weight-bearing flexion should not be done under any circumstances.
Also, unfortunately for the large population of back pain sufferers the McKenzie method is felt by some clinicians to be inadequate:
“To carry out the mechanical spinal assessment described by McKenzie requires considerable education and clinical experience; clinicians must learn the many variations and combinations of spinal movements that enable accurate assessment of a wide range of patients…Regardless of the type of onset, the well-trained clinician can identify the correct direction of end-range spinal bending that centralizes and abolishes the pain in the majority of patients.”(30)
The O’Connor Technique ™ differs substantially from the McKenzie technique because, among other reasons, it does not require considerable education or clinical experience and can be performed by the average person rather than requiring a “well-trained clinician” because it is designed to address, in a comprehensible manner, the overwhelmingly most common cause of back pain–disc disease due to disc herniations. It can be easily understood by non-medically trained people because it is based upon a few principles that once understood can be applied to nearly every activity of daily living to prevent back pain; and, above all, costs nothing. Alternatively, one can always count on spending a lot of money if one must rely upon a clinician with “considerable education and clinical experience” as described above.
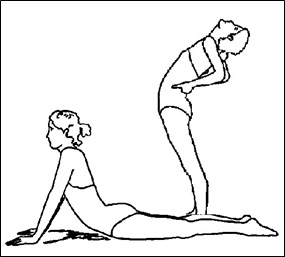
Figure 6; McKenzie exercise instructions that injudiciously promote weight-bearing on the affected disc.
I feel the need to delineate that there are multiple distinctions of substantive significance between The O’Connor Technique ™ and McKenzie’s method. The first seems to come from McKenzie himself. Clinician’s who have recently heard him speak(31) state that he argues against the distinction of having created any “McKenzie Technique” since the method relies upon the individualized creation of specific exercises for each different patient depending upon the patient’s pain pattern. By that, it does not lend itself, by his own admission, to popular use by lay persons. It requires a complex series of tests administered by a clinician who designs specific exercises which require a great deal of sustained exacting activity.
I am compelled to also point out that McKenzie, in his book, advocates the practice of actual exercises, which to my mind are not absolutely necessary to relieve back pain. Of utmost negative significance, the McKenzie exercises ignore the resistance generated by the weight of the body part(s) above the lesion in designing the selective exercise. One may note that in each of the terminal components of the McKenzie exercises, (See Figures 5 & 6), the Lumbar disc units are bearing the weight of the body parts above them. This practice is antithetical to my understanding and recommendations because it can aggravate symptoms, increase pain, and lead to disc damage (extrusions) that otherwise wouldn’t have occurred if practiced without proper insurance that the disc material is properly positioned before attempting them.
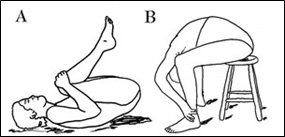
Figure 7; Flexion while weight-bearing serves to aggravate pain.
Figure 7A shows a particularly contraindicated exercise promoted by both Williams and McKenzie. The posture recommended by McKenzie in Figure 7B should, likewise, never be allowed, let alone advocated, in a patient with low back pain due to disc herniation. The reasoning for not performing these exercises and those shown in Figure 8 will become manifest later, but suffice it to say that anyone with disc disease practicing these exercises can expect to increase and prolong their discomfort.

Figure 8; Examples of physician-recommended exercises excerpted from a handout that are usually painful and never advocated in this book.
No true exercise involving weight-bearing flexion of the involved painful segment of the spine is recommended or allowed with The O’Connor Technique ™. You see, prior “wisdom” a la Williams has drawn a connection between lax abdominal tone and back pain. Probably, this association arises from the recognition that a substantial percentage of back pain sufferers have “pot-bellies.” Increasing abdominal tone (by performing sit-ups or sucking in the gut) has the effect of flexing and straightening the Lumbar spine. According to William’s and much of the current philosophy, a straightening of the spine is the ideal to be sought in an attempt to “stabilize” it. Therefore, they conclude, strengthening and increasing the abdominal musculature’s tone must improve the condition of the spine. I view their reasoning as faulty and this opinion is supported by studies which make it increasingly clear that Lumbar extensor strength is more important than abdominal muscle strength in patients with low back pain.(32),(33)
Instead, I am forced to argue the opposite! Keeping the spine “straight” may even predispose to greater harm. Biological systems do not always satisfy teleological argumentation because what appears to be the obviously logical conclusion to a set of understandings may turn out to be wrong. In biological systems, it is better to attempt to explain reality by starting with a known fact and using logic to explain the fact rather than the opposite mentation–trying to use logic to arrive at a biological fact. More often than not, this turns out to be an exercise in wishful thinking rather than science.
Human biological systems are complex, and simple logic doesn’t always apply because there are many unrecognized variables that can modify the conclusions that would otherwise appear obvious. In this instance, I can prove for myself that certain exercises can be actually harmful for persons with disc disease. I know by viewing my CT scan that I have a herniated disc at the L5-S1 level to the right. When I do a sit-up or toe-touch as advocated in Figure 8, I get pain; and I can feel the disc material go “out” and pain radiates to the right hip/buttock region. I can get out of the pain with one of my maneuvers, and I can feel the disc material go back “in” followed immediately by pain relief. The pain is located at a site wholly consistent with what the CT scan indicates. My conclusion, based on enlightened observation, is that weight-bearing flexion exercises are pain-inducing due to their displacement of disc material.
There is an exceedingly small probability that all this can be explained by some other mechanism; however, I find that difficult to substantiate when I apply the same mechanical reasoning to the overwhelming majority of my patients with disc disease who get pain with sit-ups and toe-touches then, they find immediate and repeated relief with The O’Connor Technique maneuvers. Thereby, these personal experimental observations and results become reproducible, constituting “scientific evidence.” This experience solidifies in my mind that sit-ups are contraindicated. I happen to find this reasoning far superior to handing a patient a set of painful exercises and concluding that the patient is a malingerer if he or she doesn’t practice them.
However, my experience has not yet had the opportunity to affect the many physicians and physical therapists, acting on faulty logic, from advocating these exercises; nor, when they are refused to be performed by patients who find them unnecessarily painful, from characterizing the patient’s reluctance to engage in them as emanating from a lack of motivation. Too, if a patient refuses to exercise, then they assume that there must be something wrong with the patient. With their ego-logic, it is inconceivable that the sit-up component of their exercise regimen is in error because that is not what they have come to accept as a fact through their educations. You see, clinicians are didactically taught that the classic back pain exercises help people. They reason that they must have produced a beneficial or they wouldn’t still be taught. Therefore, the illogic follows: because patients improved, they must have gotten better because of the exercises. They seem unable to modify their belief structures so as to accept as a fact that the patients get pain and could actually be hurt from that exercise. Rather, they rationalize a psychological component to explain the patients’ behavior. I find that type of logic erroneous and unfair. It doesn’t seem to dawn on them that the patients who did get better may have been getting better in spite of the exercise prescription; and, for those that were getting worse, it may have been because of them.
Also, as alluded to above, when lifting or squatting, the other programs make nearly universal recommendations to keep the back “straight.” Realistically, when a person with a disc problem attempts to follow this advice, lifting is still painful because when squatting, in order to keep the body’s center of gravity over the feet, the back naturally goes into flexion when the buttocks gets close to the heels and the hands get close to the ground. When a person attempts to keep simply a “straight” back while initiating the full squatting posture to lift, the thighs press against the abdomen forcing the Lumbar spine into a flexed position (especially if they have something more than a model’s abdominal girth.)
The O’Connor Technique ™ advocates employing a judicious extension prior to lifting and the locking of the involved area into an intentional extension posture during lifting so long as pain is not reproduced. If the pain is reproduced, then a series of specific maneuvers are taught to stop this pain so that the extensions can be accomplished safely and intelligently. The justification for these deviations from the usual and historical advice will become apparent later, but suffice it to say: This is not just another “same old, same old, back pain instruction manual.”
Not An Exercise Program
In fact, The O’Connor Technique ™ is not predominately an exercise program at all. Although the value of proper exercise to keep the back musculature in good tone cannot be underestimated as a preventative measure, it is not necessary to exercise pain away. Pain is alleviated by a few simple movements called “maneuvers.” The only actual exercise advocated in this methodology is designed to preferentially strengthen specific muscle groups to alter the mechanical forces placed upon the involved discs after the pain problem has been solved. For those who can’t see themselves being sentenced to perpetual exercise, the exercise component can be ignored and the majority of benefit can still be realized by just doing the maneuvers (some of which are so simple as to be incorporated into the act of exiting a bed or putting on your shoes in a different way.) The reader will not be expected to exhaust him/herself especially while in pain. In that sense, this website can be looked upon as the lazy (wo)man’s guide to back pain.
This method teaches the back pain sufferer a means to capitalize upon simple body mechanics to re-position the discs to relieve acute (immediate, short term) pain and to alter the forces of the spine acting on the discs so that the disc can be re-positioned and eventually made less likely to become painful in the future.
Other programs (especially those in vogue now) would have the participant repeatedly exercise and “work harden” the spinal and associated musculature in order to “stabilize” the Lumbar spine. Their latest advice recommends mobilization as early as possible. The problem is that they fail to elaborate or define specific, safe, effective, and painless mobilization techniques. This method provides those techniques and avoids any muscular stresses to the spine until the mechanical problem is solved. I find it cruel to mobilize an acutely painful back with the traditional methods especially if they make no effort to avoid those movements and postures that serve to increase pain and advance damage. The average physical therapist employing the state-of-the-art work hardening techniques seeks to find (largely through trial and error) a few exercises the back pain sufferer can perform and force them to repeat and increase the intensity of those exercises until exhaustion or pain arrests the process. All the while, they teach the sufferer to keep the back positioned in the “straight” or “neutral” position. The so-called “neutral” position being described as having the upper body directly above the hips with the Lumbar spine in neither flexion nor extension when performing any body movements. This is all well and good in theory; but, in practice, it is nearly impossible for the average person to maintain the degree of muscular energy that is required to keep the back constantly “straight.” Later, the muscle tone that they demand cannot be achieved or maintained without exhausting constant daily work-outs. Realistically, the vast majority of people do not have the inclination or time to exercise daily. Those people who do have that inclination and keep their bodies in excellent tone and shape with regular exercise usually don’t suffer from back pain anyway. This therapeutic regimen, in that sense, makes no demand for a change in exercise lifestyle.
Adding to that, most other programs and physical therapy regimens ask people who are in or just recently coming out of acute pain to risk further agony by exercising within two days of the injury! Most people are smart enough to avoid exercising because they know that, often, exercise was what brought on the pain in the first place. As you will probably be convinced later, exercising while the disc is herniated or prolapsed really shouldn’t be accomplished. As soon as it is “in,” is a different story. Any actual exercise intended to strengthen muscles acting upon the spine is too painful to accomplish until the herniated disc has been anatomically re-positioned where it belongs. Even if one were to make a constant conscious attempt to maintain the postures advocated by most programs while sitting and standing, it is largely impossible to accomplish these even most of the time due to the pain accompanying the displaced disc material. The result is that the person’s back pain persists; and, when they continue to complain, they are accused of not maintaining the postures and exercise levels consistent with sufficient motivation to get better. What their persecutors don’t realize is that the positions that they advocate are realistically impossible to maintain without first insuring that the disc is not still herniated or prolapsed.
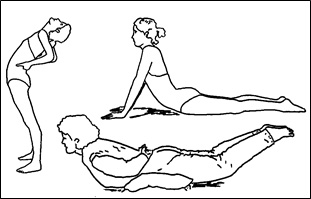
Figure 9; McKenzie exercises adapted from this text.
This rationale, as you will hopefully come to understand, substantiates a legitimate criticism of The McKenzie exercises. Figure 9 shows the terminal components of several exercise postures advocated by McKenzie that comprise principle elements of his program. In and of themselves, they are not necessarily bad (in fact, you will find similar positions demonstrated in this website); however, the inappropriate sequence of their application, as directed by his method, can make them actually painful and damaging to a large percentage of patients with disc disease a significant proportion of the time. In order for them to be helpful, a person must be able to tell whether the disc is “in” or “out,” where the displaced disc material is located (or they might be at best ineffective), and they must be applied at a specific time for rational reasons. To my admittedly limited understanding, McKenzie gives his students and readers none of this; therefore, anyone advocating these exercises lacks the necessary specificity for them to hope to be successful except under limited circumstances.
Getting Better As A Process
Making Your Bad Back Better is, among other things, an ongoing continual process of altering your activities of daily living in a non-inconveniencing manner. Take heart, though, any inconvenience can be seen to be vastly overshadowed by the benefit. The process begins by accepting that your painful back is “bad,” imperfect, damaged, broken, and/or impaired. The permanent nature of a disc problem is revealed in the studies showing that 40% to 85% of back pain patients will have recurrences within a year after their initial episode.(34),(35) The underlying problem doesn’t go away. I contend this statistic need not be the fate of a person who accepts that their back has a problem and actively uses The O’Connor Technique ™ to prevent a future occurrence.
Like any person who has encountered a disability on the long road of life, in order to overcome it, it is necessary to accept it as a disability (just ask any alcoholic who has been through Alcoholics Anonymous) because it is impossible to accommodate to something that you do not accept as real. Therefore, I would ask the reader, herewith, if you have back pain significant enough to have altered your lifestyle (even for a short period of time), that you accept the fact that your back is “broken” and that you technically have a permanent underlying disability. If you recognize this early on and you re-arrange your lifestyle to accommodate to the disability, then you will have less probability of injuring your back in the future to the extent that you are in perpetual pain or require an operation to come anywhere close to being normal again. I am certain that, had I known the onset of my back pain meant that I had actually torn the back’s non-healing structural elements, and that, if I were to sustain another flexion injury, it could mean a lifetime of pain, I would have been less likely to have participated, later, in those activities that put my back at additional, unnecessary risk.
Part of the reason I am producing this website is not only to relate how a person can get out of pain by a never-before-elaborated method but to communicate the type of information people require to prevent a similar tragedy as my own from occurring in their lives.
Had I known that my discs were weakened as a eighth grader from hauling two five gallon pails of water through Ohio farm snow drifts twice a day to bring water to our cow I would have been less likely to have launched an ultimately insignificant career in high school wrestling. During wrestling, had I known that the reason why it was necessary during warm-ups to have my back “cracked” to increase my flexibility and decrease my discomfort was because I unknowingly was getting relief by undergoing a traction/extension maneuver to centralize my own discs, I most probably would not have gone out on a mat to again lift another squirming human being over my head from a seated position. I had no idea, then, why my back hurt; and I made no effort to alter my activities even though I had found it necessary to avail myself of the services of a chiropractor at the young age of 17 years.
I had no knowledge as I aged that the small injuries I sustained as a youth were permanent and my back was a flexion accident just waiting to happen. I had no clue then as to the significance of my first flexion-type back injuries while in the military. I had not the knowledge I have now. Had I had it when I was preparing to jump off the diving board, as high into the air as I could, to do a cannon ball and land with my back in maximum flexion, I know I wouldn’t have done it. Off hand, I would categorize the avoidance of cannon-balling as a non-inconveniencing life-style change. Incidentally, that was the first incident in my life where the back pain was so intense that I was unable to get out of a swimming pool.
If someone had explained the mechanisms of disc damage to me before I bounced down a mountain in a ski racer’s tuck, I wouldn’t have spent the next several weeks in agony. This was the second incident of excruciating back pain I could recall. Had I the knowledge contained in this writing, I would have deferred the wrestling, the cannonballs, and the downhill ski racer image of myself. That is not to say that I still don’t wrestle around for fun, dive, or downhill ski. I, and almost anyone with a bad back armed with the knowledge in this website, can do just about whatever they want to, within reason; but, if they do it with the fore-knowledge that their backs must be guarded from flexion, kept in extension, and with particular purposed avoidance of weight-bearing flexion, they can accomplish these activities with relative confidence and safety.
The presence of extreme pain cannot be the only motivating factor because, by then, it may be too late to prevent extensive damage. If you wait till you have pain to allow it to protect your back, the opportunity to prevent the damage is passed. After incorporating this methododology into your lifestyle armamentarium, you can let your newly acquired intellect decide what constitutes a wise move. If you are capable of assimilating the knowledge and experience of others and not the type of person who requires actually experiencing a negative event from which to learn, you will do well with your back.
If this website does significantly help you and you are convinced that the source of your pain is indeed a displaced disc, please don’t adopt a maladaptive attitude towards yourself. If I may be given the latitude to wax philosophical, one must not look upon any constraints on your behavior as punishment, as a shackle or enforced prison. Not as a disgruntled malcontent should you look at your body. Regardless of its failings and imperfections, it is still the temple of your soul. It’s the only housing your being has for the present. It is what it is for whatever reason. You would do well to accept this “disability” as though you are a child issued your first set of prescription lenses, or as an elder your first prescription medicine which will be taken for the rest of your life. You must understand that Fate is an inscrutable mistress. She may dictate through your back that your chances of sustaining a flexion injury are enough to encourage you to walk away from a boisterous argument that years prior you would have confronted and otherwise put your life at risk. Believe it or not, as a teenager, I distinctly recall recognizing that my back pain would preclude my relying upon a career involving physical labor. That realization led me to invest more in my mind and, rather, cultivate my intellectual capacity.
I’m not advocating adopting a “Pollyanna” perspective, I’m just exposing you to the reality that you will never know (until perhaps the last second of your life) if your back pain was ultimately a beneficial happening. From all immediate perspectives it appears singularly disastrous; however, you never know, it may save your life someday. Funny thing is about Fate, you may never even know how or if your back saved your life. I know that my other disability, my glasses, saved my life. In an impulsive teenage heroic mentality, I had applied for the Warrant Officer Flight program in 1969 so that I could be a helicopter pilot in Vietnam. The prescription lenses that I cursed every day of my life excluded me from “going out in a blaze of glory” at the ripe old age of twenty years.
Certainly it is depressing to realize that your body is disabled to the extent which accommodations must be made for the rest of your life. Just talk to someone with an amputation or a stroke survivor, you will find that the successful ones simply accepted their “disability” and went on with the rest of their lives by making the necessary modifications to their lifestyle. However, there is good reason to expect that your back will eventually get and stay better especially if The O’Connor Technique ™ is adhered to. The reader can breeze forward to the section on “HOPE” to reassure themselves that there is some light at the end of the back pain tunnel so long as you can bring your spinal education level up to the point where you can understand the terminology and practice the methods designed to accomplish the few principles enumerated in this website.
Applying The O’Connor Technique ™ supplies a means whereby a person who is predisposed to back pain by genetics, comes to it by occupation, prior accidental trauma, or pregnancy, or has had a previous event of back pain (and wishes to prevent future ones) can alter their behavior with a process designed to protect their spine before the onset, during the period of pain, and subsequent to it. In this manner, The O’Connor Technique ™ can be said to be able to prevent back pain and change the Fate of one who practices it.
The principles are especially relevant to those who are wise enough to foresee the probability of acquiring back pain, decide not to expose themselves to that risk, and are willing to change their mechanical behavior to accommodate this desire. It requires wisdom to prevent future pain because rarely is it possible to convince someone, even with the best of proof, that an untoward event would have happened if it didn’t or never does happen. That is what makes preventive medicine so difficult for some to accept as valuable. After all, they contend, one could theoretically be expending a great deal of extra effort trying to prevent an event that may never take place; however, when the reader gets pain relief using a maneuver in this website, it is easily seen how the maneuver is based upon spinal mechanical principles that make the maneuver successful. It is from consistently applying this same mechanical logic that the process of preventing future pain is designed. The more effort generated towards obeying and applying the principles, the less probability one has of committing the mechanical errors that lead to back pain and disability.
The permutations and levels upon which this preventive strategy operate are farther reaching than just immediate pain. For instance, knowledgeable of spinal realities, new mothers can use this process to insure that motherhood doesn’t turn into an experience that taints the life long relationship with their new child. To estimate the value of that benefit, imagine a scientific experiment wherein every time one study group of new mothers bent over to pick up their baby they get a jolt of pain stabbing them in the back. It takes little imagination to predict how such a scenario could potentially breed a subtle psychological form of resentment directed at the child and dis-flavor the relationship as the mother subconsciously associates the infant as the origin and source of the pain. Applying the principles of The O’Connor Technique ™ serves to prevent this potentially devastating ramification of pain.
I am firmly convinced that, had someone communicated the wisdom contained in this website to me as a juvenile when tossing hay bales to the point of exhaustion, as an adolescent while slouching for hours in my school chair, or as an adult trying to squat like an Asian while in Vietnam (mistakenly thinking it to be a natural and therefore biomechanically advantageous position), I would have understood how and why these activities were making and made my back worse; and I would not have persisted in them. In that sense, had I the wisdom to apply this intellect, my Fate would have been irrevocably altered by simple preventive medicine.
Armed with and applying this wisdom now, as a physician, when patients walk into my office in pain, I determine through a brief history and specific physical examination whether a disc is acting as a source of the pain, apply my technique in a manipulative manner, and they walk away with immediate relief after the application of gentle movements which could only result in a disc’s re-centralization. In all those persons who obtain relief, the specificity of the therapy’s efficacy proves the diagnosis. The objective evidence is that, after the application of The O’Connor Technique ™ the patient can again move without the stabbing wedge-like pain in their spine with which they entered my office. With that experience, they are much more motivated to accept and apply the preventive philosophy I then impart to them. It has proven to be an intensely gratifying experience to know unequivocally you have taken a person out of pain, unequivocally given them a means of preventing its return, and changed their Fate, forever. The reader of this website can expect to do the same for him or herself.
I have no illusions that this self-applied “physical therapy” process will help everyone. However, I am so convinced of its efficacy, that those that it doesn’t help have reasonable cause to assume that they have some other condition like those listed above or the disc is in such a difficult position that it cannot be self-manipulated back into place .
Fortunately for most physicians but unfortunately for their patients, they don’t have personal experience with a disc problem upon which to base their belief systems. That, in the presence of never before being exposed to this technique nor the mechanical theory of disc movement upon which The O’Connor Technique ™ is based, leaves them with little to rely upon except the customary, random, back mobilization exercises which, by the laws of random activity, do eventually help a percentage of people. Because some studies indicate that 95% of acute back pain resolves in 2 months no matter what modality of therapy is utilized, many practitioners simply give analgesics (pain medicines), anti-inflammatory medicines, some bed rest instructions, an admonition not to lift, some largely worthless exercises, and rely upon time and the law of averages to do the real work. The O’Connor Technique ™ is refreshing in that it removes randomness from the process by selecting out those who most probably have a disc herniation as the source of their pain and mechanically re-positions the disc material so as to immediately resolve the originating component of the pain and teaches the process of keeping it in.
Become Your Own Chiropractor
Chiropractors for years have explained their technique as one in which the manipulator “adjusts” the spine. The theory (as explained to me on numerous occasions when the nearly identical “spiel” is repeated in offices, at street fairs, etc.) holds to a belief that the spinal vertebrae can go out of “alignment.” The chiropractor usually demonstrates this condition with a spinal model whereupon he rotates one of the vertebrae so that one edge of a facet (the joint type structure that constitutes a posterior aspect of the vertebral bone and acts to keep one vertebral body directly above or below the next) rests on top of another which then stays in that position until he re-rotates the spine in the opposite direction and the vertebrae falls into place. This action is to what they give credit as the source of their ability to relieve spinal pain, not to mention any other malady to which the body falls prey. I’m not certain whether even they truly believe it or not, however some seem pretty convinced and convincing. Maybe they are just repeating the same rationalization over and over (despite a knowledge that it cannot really explain the spine’s mechanics) because they have to give some reason to justify a rapid and violent jerk to the torso and the wallet. However, it could be that they do have a knowledge of the true mechanics of the back yet understand that, if they reveal it to others, the majority of patients will figure out how to accomplish the same effect on themselves and eliminate the chiropractor along with his compensation.
Most physicians with a knowledge of spinal anatomy and function cannot accept the reasoning many chiropractors give as an explanation because it is blatantly obvious to them that the forces necessary to allow a vertebrae to assume that “misaligned” configuration would have to tear all the ligaments designed to prevent that action from occurring. Too, the degree of the misalignment has to be of such magnitude as to have occurred due to forces far beyond those reported as precipitating the painful event. Certainly, trauma on par with an auto accident could create such stresses; however, it is highly unlikely that 1) the interarticular ligaments could sustain such injury and still allow the spine to function at all, 2) that such a mis-alignment would not be obvious on X-Ray, and 3) once the vertebral column was re-aligned it would scar down and prevent further misalignment unless equivalently violent forces were again to act. This discrepancy between theory and observed reality, compounded by the seemingly arbitrary assignment of repetitive future alignments that appear to be more monetarily motivated than physically beneficial, probably is responsible for the failure of most medical doctors to accept chiropractors as legitimate therapists.
On the contrary, I possess the objectivity to recognize that chiropractors do help some people. Statistically, about a third of the people they manipulate get relief; however that only meets the batting average of a good placebo. Since there are only three possibilities that can result from any given therapy; the patient 1) gets better, 2) gets no effect, or 3) gets worse. I assume that the percentages for each option are about equal. When chiropractors go through their routine, they simply spin a three sectioned wheel of probability. The times that I have been “manipulated,” it didn’t seem to matter what my problem was, the treatment was the same. My back did feel a little better afterwards, some of the stiffness was relieved as the successive crunching was accomplished. But the problem was not addressed in any long-lasting or permanent manner.
This should not be taken to mean that they do not actually accomplish something that physically helps other individuals. I am only saying that I think they are attributing the relief, when it results, to a mechanism that they admittedly (in the literature) do not understand. Therefore, they should not take credit for their successes as a science since it is not the product of consciously directed action based upon intelligent thought processes. The possibility also exists that they are leading people to believe it is a different mechanism for some alternative reason, acting under the assumption that, if the true mechanics were explained, the patient could do the equivalent movement at home to themselves and, thereby, not need to repeatedly visit a chiropractor).
Their ability to help people then, to my assessment, becomes a process of simple therapy-mediated (as opposed to diagnosis-mediated) patient selection, whereby, those with minor disc herniations that are amenable to the chiropractic forces generated when the back is literally “wrung” by force, are helped. Those that do not have such simple lesions are eliminated with respect to the probability of future benefit. This causes me to contend that a certain set of patients actually do get true short-term relief because, in the twisting action of chiropractic manipulation, the disc is effectively (albeit violently) shoved back nearer to a more central position when the ligamentous structures holding the vertebral bodies together are tightened in a partially unweighted position. Regardless, it is not because someone figured out what was mechanically disordered through a diagnostic process and formulated the ideal therapy. It is more the product of myopic (in contradistinction to “blind”) luck whether a person is helped or not.
It is technically fraudulent to classify chiropractic as a “science;” however, this is not to say that twisting a persons spine in a standard manner will not carry some level of success. Manipulative therapy is described by chiropractors as “the art of restoring a full and pain-free range of motion to joints in order to counteract the harmful local and distant effects of hyper- or hypo-mobile joints that have wide-ranging consequences on other parts of the body.” They deliver a “high velocity but low amplitude thrust” that, usually, if successful, causes a usually painless, audible noise. In so far as I am concerned, the audible clunk, or crepitation that is heard is the fibrocartilaginous material crunching past other fibrocartilaginous material within the disc space. I have good reason to believe that it is the same sound often heard during the performance of The O’Connor Technique ™ MANEUVERS.
A 1989 study reported that “the public seemed to be more satisfied with chiropractors’ level of understanding of the problem of the spinal patient’s problems and more confident with the diagnosis and management when compared to family practitioners”(36). These data suggest that the family practitioners were not able to provide as clear or rational an explanatory model of the problem as chiropractors. Considering that chiropractors themselves readily admit that they cannot explain how manipulative therapy actually functions mechanically, anatomically, or physiologically, these studies imply only that chiropractors are more expert at perpetrating misrepresentations than family practitioners. It demonstrates to me that chiropractors do not help alleviate back pain better but simply are better able to “con” patients into believing that they know what they are doing, and family practitioners are equally as ineffective but more honest in their responses.
A societal casualty of this study’s misinterpretation is the published conclusion: “The message here is pretty clear: since most patients are going to get better regardless of the treatment they receive, how we (physicians) treat the pain is less important than how we make patients feel about their care.”(37) To hear that sort of conclusion evidences to me the sorry state of 1990’s back pain management and a more obvious finding. It would appear that physicians are willing to concede that chiropractors are better at deceiving the public than they are and that doctors should learn to engage in similar practices so as to deceive patients equally well if not better. Such logic makes me lose faith in the competence of those researchers entrusted with the duty to adequately interpret scientific data and draw competent conclusions.
In my opinion, the message should be something more akin to: physicians are doing a horrible job of helping people with back pain and rather than learn how to dissemble better than chiropractors, they should redouble their efforts to find a method that actually helps people rather than creating an illusion of expertise while letting the patient walk out the door with only the law of probabilities on their side.
The O’Connor Technique ™ can elegantly satisfy that need without resorting to hand-holding hocus-pocus. If you achieve substantial benefit from this website, I would suggest you inform the health care provider who failed to adequately alleviate your pain of this website’s existence, so that they can, as rapidly as possible, begin to engage in meaningful discourse and treatments before they degenerate into chiropractic coddling. In the long run, true trust might be developed.
In deference to the field of chiropractic and to present a balanced picture, there are several controlled trials that provided evidence that chiropractic manipulation has a beneficial effect for low back pain, especially for select subgroups of patients; however in a study of 35 randomized trials of manipulation, only 5% showed an improved short term outcome, again though, selection biases and lack of standardized diagnoses make even that success profile subject to interpretive bias that evidences one already largely known marketplace fact: Some people do get relief from chiropractors.
What is problematic about their “theory” and practice is that they promote the belief that they can treat any number of unrelated diseases and that a long term management plan is necessary that causes a person to return again, and again, and again, for complete treatment success. In fact, they cannot consistently or scientifically fulfill those representations. Getting people to believe that a long-term, repetitive, practitioner mediated process is necessary accomplishes at least one thing–it insures a steady income for the chiropractor. Leading the patients to believe unrelated allergies or ear infections can be remedied by crunching on a spine, in my opinion, constitutes fraud and any chiropractor that strays into this realm should be abandoned in favor of one who sticks to helping the percentages of patients that they do help with spinal pain.
It is my belief that, in the future, when the principles of this method are widely studied for confirmatory validation, the chiropractic beneficial effect will be anatomically demonstrated to be slightly similar. In those few patients who have ideally-placed pieces of displaced disc material in the Lumbar or Cervical regions the herniated disc material can be serendipitously repositioned centrally by the wringing action of tightening the ligamentous peripheral lamina of the annulus fibrosus rapidly and forcefully during the twisting-type chiropractic manipulation very similar to the means described in the chirotational TWIST Section of this website. If this doesn’t produce instant relief or if the lesion is in the less rotatorily mobile thoracic spine, another manipulative technique is employed in which the spine is put in slight traction by positioning; then a sharp, forceful push with the palms is given to the spine which induces an immediate hyper-extension. This, too, is similar to the non-weight-bearing extension principle described in the EXTENSIONS Section of this website which physically squeezes the disc material anteriorly, so long as the disc material isn’t positioned too far peripherally. If so, the pinching can squeeze off a partially extruded disc segment; and turn it into a fully extruded or sequestered fragment. Therein lies the harm they can do.
Their limited success rates can be explained because there are only certain small percentages of displaced discs configured ideally to be helped by conventional chiropractic manipulations and, I would argue, that these are the only patients who are benefited and, then, only for the short term. This commits those select patients who “swear by” instead of “swear at” chiropractors to a lifetime of repeated remissions requiring costly subsequent treatments. Until the advances made by The O’Connor Technique ™ are put into widespread practice, without chiropractic treatments, these patients would still suffer; so, chiropractors do provide a legitimate service.
It is humorous (if not absurd) in this supposedly scientific era to recognize that chiropractors themselves admit that they can’t (despite years of education) competently describe or explain adequately the means by which their method works; however, I do not deny them their successes in the above described context. The charade begins to be exposed when, before accomplishing the manipulation, scarce real efforts are made to truly diagnose those who definitely will be benefited by the treatment. Too often, there is scant effort directed to select out those who most probably will be further injured by the process because that would be turning away “business;” however, in all fairness, I have received a number of chiropractic referrals because the chiropractor did legitimately recognize a nerve impingement before initiating treatment.
In order to make the proper assessment, I can see no other way for them to safely persist in these practices unless they apply the theory and practice of this method or resort to routinely using CAT Scans, NMRI’s, or Myelography to determine, in advance, the precise location of the disc material relative to the spinal nerves prior to the application of exogenous force. However, it would be unrealistic for them to attempt to convince patients to spend hundreds of dollars to insure that their manipulations are safe; so, they must just keep “cranking” on backs to see what happens. In an almost Darwinian selection process, only the “fittest” survive their culling and the rest are left to Nature’s sometimes cruel alternatives.
You see, in order to achieve their limited success rates and therapeutic results, it is necessary for chiropractors to generate a certain high level of torque force to be effective on that percentage of backs that they do help. It is the act of applying that equivalent level of force injudiciously that gets them into trouble. Most apparently don’t disseminate statistics upon how many patients leave the office in greater pain than when they entered.
Instead, most patients are given basically the same gibberish about a nebulous “subluxation” causing an aggravation of nerves having effects on any number of distant, anatomically unrelated organs or tissues, lain on a table, and given the same hand-on-shoulder and hip-twisting of the spine procedure given to everyone else who walks in the door. This may be accompanied by some different hocus-pocus with measurements of the legs, levels of the shoulders, or expensive (largely useless) X-rays. This practice wouldn’t be so bad if they didn’t usually buy-up old X-Ray machines with higher radiation outputs than are allowed to be sold today and unnecessarily expose their patient’s sexual organs which are particularly sensitive to radiation damage. One needn’t accept my word on this score, according to a recognized authority on the spine, Dr. Richard A. Deyo: “Spine films are of little use in making a diagnosis, and they are costly and expose patients to significant radiation directed right at the genitals.” One would do well to consider the risk/benefit ratio of spinal X-rays before consenting to them.
My knowledge of the spine gives me reason to believe that a wrenching maneuver of the spine could quite reasonably result in a worsening of the patient’s condition. If the herniation has progressed to the point where the disc material is on the verge of or has actually escaped the joint capsule, then the action of twisting can squeeze the fragment further into the canal resulting in a sequestered fragment or, worse, can shove the fragment into a nerve root. This can change a condition from not necessarily a surgical condition to a surgical necessity.
No statistics of which I am aware have documented the number of people who have had borderline discs turned into surgical cases due to forceful manipulation. In fact, it would be very difficult to do so because it would require an NMRI or CT scan in advance of going to a chiropractor. Then, after the damaging event, the patient would have to have a repeat NMRI or CT to document the disc material’s movement. Such a study would also have to demonstrate that the disc did not get worse on its own. Such a study would require the coordination of a chiropractor and a neurosurgeon such that the chiropractor anticipated that he could make a particular patient worse and, immediately after he does, sends him to a neurosurgeon. Alternatively, thousands of patients going to chiropractors would have to have a CT or NMRI immediately prior to and after such an event. The former would never occur because no reasonable chiropractor will expose himself to the potential lawsuit resulting from a condition he knew he made worse in the presence of an anticipation to do so and the latter would be so expensive as to be prohibitive. So, the requisite science to provide this information does not appear to be forthcoming in the immediate future.
The O’Connor Technique ™ doesn’t fall into this trap because, largely, through self-manipulation, the patient is able to control the direction and level of force at all times, which they can automatically stop before it becomes too painful to cause damage. No rapid torque is required to achieve the same results in nearly all the people who would otherwise be actually helped by chiropractors. In that sense, the reader of this material can, more safely, become their own chiropractor and more.
Personally, with those patients I manipulate in the office, I could not bring myself to do such a forceful manipulation without knowing the anatomy of the problem for fear that I could possibly make the patient worse. A simple X-Ray would not accomplish this necessity because it doesn’t image soft tissues and the non-bony disc material does not show up on an X-Ray. The CT and the NMRI do so, but they cost around $1000. No other imaging study short of a myelogram (a painfully invasive X-Ray that places dye into the spinal canal) would show the proximity of the disc material to the nerve root and thereby ascertain manipulation’s safety.
So, chiropractors largely approach the condition blindly or at best with such poor acuity that, to me, constitutes a potentially dangerous form of individualized human experimentation. If they perform the same manipulation on everyone, the ones that get better will come back, and those that are hurt worse presumably won’t. When the people who do get worse don’t come back, the chiropractor assumes they are better if he is an optimist, but rarely will concede that they may have gotten markedly worse unless he is taken to court.
Luckily, the low back is relatively forgiving when it comes to the damage a chiropractor can potentially do; but, when chiropractors attempt to manipulate the neck, especially in the elderly, the vertebral artery’s actual passage through a hole in the transverse processes of the cervical vertebrae and/or the tension put on the carotid artery can lead to a stroke.
A recent report presented at a stroke conference sponsored by the American Heart Association, at which several specialists said they had treated patients’ arteries torn during sessions with chiropractors, described “probably the best documented cause of rips–what doctors call dissections–is chiropractic manipulation of the neck.” At the conference, Dr. William Powers of Washington University in St. Louis said “every neurologist in this room has seen two or three people who have suffered this after chiropractic manipulation.” It was also stated that 85% of cases result in at least mild impairment according to a Stanford survey.(38)
The O’Connor Technique ™ differs substantially from chiropractic in that no forceful movements or manipulations are necessary or advocated. Success in alleviating pain does not rely simply upon the actual movement or forcefulness of the effort with The O’Connor Technique ™ but with the proper sequential combinations of movements that are revealed herein. Forcefulness is not necessary to open a lock if one knows the combination.
The patient performing the MANEUVERS controls the amount of force and can stop the maneuver at anytime pain occurs. The time taken to relax necessary muscle groups and allow the components of the annulus fibrosus to accept traction is an individualized process that the individual determines. In those cases where this technique would be equivalently as successful as chiropractic, the same end is achieved; but the cost is almost non-existent with The O’Connor Technique ™.
With The O’Connor Technique ™, most persons who do routinely get relief from chiropractors are taught to do their own “manipulation” and given the power and means to prevent future pain themselves. Even if chiropractors knew what they were doing they would be unlikely to share their “secret” because that would reduce the number of people coming back for treatment, after treatment, after treatment. For this reason, it will probably be a long time before chiropractors embrace the theory and practice of this technique and may be reluctant to teach it since to do so might put the majority of them out of business. In fact, it would not surprise me to see a rather boisterous reaction to any large-scale promotion of The O’Connor Technique ™ from some components of the chiropractic establishment.
Hope
At times, it may seem to the back pain sufferer that there is little or no hope for ever being “normal” again. Some readers may say to themselves, “If I have to go through all this every day of my life, I might just as well have the whole thing fused surgically and live with a stiff low back.”
I would strongly argue that this is the wrong attitude. Surgery should only be viewed as the very last resort for unremittant, debilitating, pain or vertebral instability when neurological function is compromised or at risk of being lost. Later in the website, you will learn that, even for people who undergo a fusion surgery or discectomy, the predisposition for additional degenerative disc disease still exists at other (especially adjacent) levels of the spine. Without intentional intervention, the damaging forces acting upon the discs will still be present and capable of inducing further future disability and pain. Quite often, the surgery is only a partial discectomy and the same disc continues to degenerate. Just because you have one disc repaired, doesn’t mean that your problems with your spine are solved. Quite the contrary, if you don’t alter the mechanics, there is every reason to believe that other discs will fall prey to the same forces that damaged the original one.
In fact, my observation has been that an inordinately large percentage of persons with Lumbar disc disease eventually present with similar Cervical or Thoracic disc problems and visa versa. This leads me to conclude that there must be certain genetic predispositions to faulty disc mechanics and that the ramifications of some inherent structural protein difference results in a weakness of ligamentous capacity that is reflected in one person’s ability to sustain the same amount of force without damage to the disc whereas another person under identical circumstances ends up with a damaged disc. I suspect it has something to do with the tensile strength and elasticity of their collagen fibers (the proteins that compose ligaments and cartilage) and that there are certain genetic subsets of persons who are destined, by virtue of their hyper-elastic collagen, to have an increased probability of disc disease regardless of whether or not they sustain major, forceful injuries. This trait may make them evolutionarily more likely to survive by giving them the “wirey” capacity to wriggle free of their enemies; but the gains they achieve in elasticity leave them deficient in tensile strength. If this is true, these people (of which I think persons with hyper-flexible joints and/or scoliosis may be an extremely affected subset) may be prevented from what otherwise appears to be an inevitable fate. However, it is too early for me to make that speculation formally; and this website is not the appropriate forum. Suffice it to say, I have enough information to advance the suspicion and hypothesis because I have observed scoliosis induced solely by disc disease. Time and wide-spread use of The O’Connor Technique ™ will determine whether this suspicion is correct. Until then, persons with early scoliosis are free to make and act upon the assumption that the origin of their disease process rests in hyper-migratory disc material and use The O’Connor Technique ™ to try to prevent disfiguration. They certainly are unlikely to come to any additional harm by practicing these techniques; and I would enjoy learning if they appear to be successful, so that a comprehensive, scientific study could be rapidly assembled to test that hypothesis. The number of scoliosis patients I currently, or ever, will see in my practice is so small as to be negligible–someone else will have to study that question.
Contrary to political rhetoric, all men are not created equal. However, that is not to say a person with a predisposition for a bad back is inferior to someone with an intact spine because having extra-flexible collagen may impart some other selection advantage and survival value. Judging from the multitudes with bad backs alive today, it seemingly doesn’t carry any Darwinian selection disadvantages. Perhaps the increased flexibility carries with it an, as yet unrecognized, selection advantage, the usefulness of which becomes less significant after offspring are successfully reared.
However, it does not follow that simply because one has a bad back that it is the result of an inexorable genetic failing. One needn’t adopt the fatalistic attitude that their Fate is immutable or that they are pre-destined to suffer or I would not have written this treatise.
Hope does exist in the peculiar capacity the human organism has for accommodation on an intellectual and structural level. Understand that acting upon knowledge can favorably change fate, and the body is not a static entity. It is constantly being broken down and rebuilt on a microscopic level. Although, to the unenlightened, when viewing a skeleton it seems to exist as a hard, rigid, structural frame that is unchanging in life as much as it is in death. Quite the contrary, even this rigid bony structure is constantly being broken down and reformed at the cellular level. This rebuilding can be modified depending upon the stresses applied. Obviously, there are certain structures that, once broken, cannot be rebuilt to their original functional capacity. There are certain conditional restrictions upon the ability of the human organism to repair damage. Yet, over time, the pre-programmed capacity of the body to modify its structure can be capitalized upon to expect eventual healing and return to a near-normal functional activity level.
A major constituent of The O’Connor Technique ™ is a fundamental methodology that optimizes the capacity of the human body to intellectually and physically adapt to spinal damage as well as maximize effective repair. These components are referred to as flexion avoidance, maintenance of extension, dynamic positioning, and preferential strengthening/selective hypertrophy. With these and other innovations in back pain management, The O’Connor Technique ™ has taken a great step forward in reducing the healing time, decreasing the duration of back pain events, and preventing or reducing the frequency of future episodes. Separate sections in the website specifically address these components and throughout the website wherever pertinent, they are reiterated in contexts where appropriate. The reader who understands and practices them can expect to have true hope for a largely pain-free future.
1. Bigos SJ, Deyo RA, Romanowski TS, Whitten RR, The new thinking on low back pain, Patient Care; July 15, 1995:140-172
2. Bigos S, Bowyer O, Braen G, et al. Acute Low Back Problems in Adults. Clinical Practice Guideline, Quick Reference Guide Number 14. Rockville, MD: U.S. Dept. of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research, AHCPR Pub. No. 95-0643. December 1994.
3. Korff, et al., Pain , 1988, 32:173-83.
4. Reis S, et al., Low Back Pain: More than Anatomy, The Journal of Family Practice, 1992;35(5):509.
5. Deyo RA, Mayer TG, et al., The painful back: Keep it moving, Patient Care, October 30, 1987:47-59.
6. Frymoyer JW, Helping your patients avoid low back pain, The Journal of Musculoskeletal Medicine, May 1989:83-101.
7. Frymoyer JW, Helping your patients avoid low back pain, The Journal of Musculoskeletal Medicine, May 1989:83.
8. Graves EJ. Diagnosis-Related Groups Using Data from the National Hospital Discharge Survey: United States–1985. Hyattsville, Md: 1987. US Dept of Health and Human Services publication 87-1250.
9. Miller S, Total Fitness Program Best for Low Back Problems, Family Practice News, June 1-14, 1989; 19(11):37.
10. Op.Cit. Endnote #1;p.140-172
11. Cole HM (ed.), Diagnostic and Therapeutic Technology Assessment (DATTA), The Journal of the American Medical Association, Sept 19, 1990, 264, (11):1469–1472.
12. Sack B, Acute and Chronic low back pain: How to pinpoint its cause and make the diagnosis, Modern Medicine, Sept. 1992;(60):58-92.
13. Vlok GJ, Hendrix MR. The Lumbar disc: evaluating the cause of pain. Orthopedics, 1991; 14:419-25.
14. Deyo RA, Loeser JD, Bigos SJ. Herniated Lumbar intervertebral disk. Ann Intern Med, 1990;112:598-603.
15. Predicting Outcome in Back Pain Patients, Family Practice News, Oct 1-14, 1986:1-36.
16. Frymoyer JW. Back pain and sciatica. N Engl J Med. 1988;31;82-91
17. Anon, Family Practice News, August 1-14, 1987.
18. Anon, Back Pain Is a Definitive Diagnosis Necessary?, Emergency Medicine; February 15, 1993:131-134.
19. Cherkin D, Deyo RA, Berg AO, et al, University of Washington, Seattle, and other centers; Evaluation of a physician education intervention to improve primary care for low-back pain I: Impact on physicians. Spine, Oct 1991;16:1168-1172.
20. Cherkin D, Deyo RA, Berg AO, et al, University of Washington, Seattle, and other centers; Evaluation of a physician education intervention to improve primary care for low-back pain I: Impact on patients. Spine, Oct 1991;16:1173-1178.
21. Kriyananda, Yoga Postures for Self-Awareness,(1969) Ananda Publications, San Francisco, CA, USA.
22. Yogiraj Sri Swami Satchidananda, Integral Yoga Hatha, (1970), Holt, Rinehart and Winston, New York, USA, p. 49.
23. McKenzie, R, Treat Your Own Back, Spinal Publications LTD., P.O. Box 93, Maikanae, New Zealand, p.9.
24. Mooney V, quoted in Backache: What Patterns of Pain Pinpoint the Source?, Data Centrum, April 1984;1(4):25-37.
25. Weber H, Lumbar disc herniation: a controlled, prospective study with tens years of observation. Spine. 1983;8:131-140.
26. Saal JA, Saal JS, Herzog RJ. The natural history of Lumbar intervertebral disc extrusions treated non-operatively. Spine, 1990;15:683-6.
27. Williams PC. Low back and neck pain causes and conservative treatment.2nd ed, Springfield, Ill:Charles C Thomas, Publisher;1974.
28. Leblan K, et al. Report of the Quebec task force on spinal disorders. Spine. 1987;12:S1-S8.28.
29. Op.cit., Bigos, Endnote #2.
30. Donelson RG, Identifying appropriate exercises for your low back pain patient. The Journal of Musculoskeletal Medicine; December 1991:14-29.
31. Weed D, Chiropractic Care, The Specialists Neck and Shoulder Injuries Lecture, August 31, 1995, Fairfield, CA.
32. Ross EC, Parnianpour M, Martin D, The effect of resistance level on muscle coordination patterns and movement profile during trunk extension. Spine. 1993;18:1829-1838.
33. Flicker PL, Fleckenstein JL, Ferry K, et al. Lumbar muscle usage in chronic low back pain. Spine. 1993;18:582.
34. Valkenburg HA, Haanen HCM. The epidemiology of low back pain, in White AAIII, Gordon SL (eds) American Academy of Orthopedic Surgeons Symposium on Idiopathic Low Back Pain, St. Louis, CV Mosby Co, 1982:9-22.
35. Troup JD, Martin JW, Lloyd DC, Back pain in industry: A Prospective Survey, Spine (1981) 6:61-69.
36. Cherkin D, MacCornack FA. Patient evaluation of low back pain care from family physicians and chiropractors. West J Med, 1989, 150:351-5.
37. Hockberger RS, Meeting the Challenge of Low Back Pain, Emergency Medicine; August 15, 1990:99-127.
38. Associated Press, Report on the causes of stroke fingers chiropractors, San Francisco Sunday Examiner and Chronicle, 2/20/94:A5.